| front |1 |2 |3 |4 |5 |6 |7 |8 |9 |10 |11 |12 |13 |14 |15 |16 |17 |18 |19 |20 |21 |22 |23 |24 |25 |26 |27 |28 |29 |review |
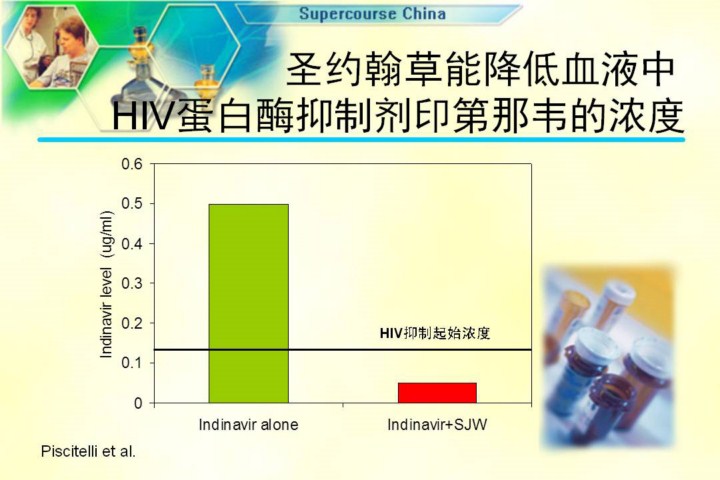 |
Judy Falloon and her colleagues upstairs on the eighth floor surveyed AIDS patients and found that the vast majority of them used dietary supplements and other CAM approaches. She and Steve Piscitelli, a research pharmacist here at the NIH, took normal volunteers and gave them one of the potent new classes of AIDS drugs, the protease inhibitor Crixivan (indinavir), and showed that taking that drug established very good blood levels, and those levels at all times around the clock were sufficient to inhibit the replication of the virus, at least in the virus. But when they added to that very dose the same dose of St. John’s Wort in the depression trial, this is what happened to the blood level of indinavir: it fell substantially to levels that, at many times of the day, would not have been adequate to inhibit the replication of the virus. So you have to ask, if it’s going to be effective, it will be effective because it, in some way, interrogates natural biochemical systems, and that produces the possibility that it will also have unanticipated risks. The question is, why is St. John’s Wort doing this? We took this as a vehicle, and as a signal to us in NCCAM, to call for applications specifically to begin to study the potential interactions between botanical products and drugs. Now, when some of these herbs were first used by indigenous people’s a thousand years ago, you didn’t have to worry whether they interacted with birth control pills or indinavir, but we do today. And this interaction is something that we’re studying through grants to about a dozen applicants around the country doing preclinical phase I and phase II studies.
圣约翰草降低HIV蛋白酶抑制剂茚地那韦的血液浓度
|