Analysis of Two Tibial Liners in PCL Retaining Total Knee Arthroplasty
D. Lung, D.J Tarinelli, MS, L. Crossett, MD, J.M Lee, MD, T.M Vogrin, MS, S.L-Y. Woo, PhD., DScMusculoskeletal Research Center
Department of Orthopaedic Surgery
University of Pittsburgh Medical Center, PA
Introduction
Surgeons retain the Posterior Cruciate Ligament (PCL) in Total Knee Arthroplasty (TKA) believing that it provides improved stability and allows femoral rollback, enabling greater flexion. There are two commonly used polyethylene tibial inserts used in PCL retaining TKAs. One is the relatively flat Posterior-lipped (PLI) liner, which is preferably used when the PCL is functionally intact. The other is a more curved liner (CVD) that is designed to provide greater conformity when the PCL has sufficient laxity. Both of the liners are designed to produce sufficient femoral rollback. My project this summer was to determine which liner provides greater rollback in a TKA. We hypothesized that since the CVD theoretically provides greater conformity, that more femoral rollback would occur in the PLI liner.
Methods and Materials
For this study we used five fresh-frozen human cadaveric knees on the robotic/universal force-moment sensor (UFS) system. Each knee was thawed to room temperature before testing. Radiographs were taken at set angles (full extension, 30, 90) and analyzed to obtain the mechanical and anatomical axes. Radiographic templates were overlaid on the films to estimate the approximate size of the prosthesis.

Figure 1: Radiograph of a CVD liner at 30 degrees.
Results
I analyzed the radiographs to determine the femoral-tibial contact point. From that point I would measure the percentage of the liner from that point to the edge at the anterior side. This percentage will increase with increasing femoral rollback throughout flexion.
Figure 2: Line graph showing the CVD vs PLI liner
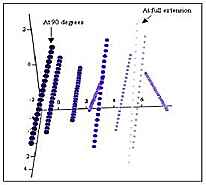
Figure 3: Screw Axes for an intact knee.
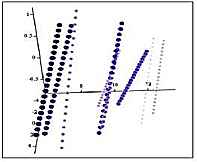
Figure 4: Screw Axes for a CVD liner
Figure 5: Screw Axes for a PLI Liner.
Discussion
The current data shows that the CVD liner provided slightly more femoral rollback than the PLI liner. Unfortunately the data from knee to knee was very inconsistent, (some knees did not show rollback at all) which seems to point to the fact that these results are not very reliable. This inconsistence showed in both the radiographs and the screw axes. The screw axes did show more precisely the femoral rollback (3D as opposed to 2D), and is more feasible than taking 9 radiographs every 10 degrees.
Future Directions
To develop a way to quantify femoral rollback using screw axes. Difficult to quantify since each knee has a different paths. Maybe a comparison with the rollback that occurs in the exact knee before the TKA is performed. Calculating rollback under loading may also be a possibility.
Acknowledgments
I would like to thank Danyel for her guidance, and all the residents along with Ted Rudy who helped during the experiments. I would also like to thank Dr. Gilbertson and Dr. Woo for giving me the opportunity to work at the MSRC this summer. Lastly I would like to thank my fellow summer students who made the MSRC a fun and enjoyable place to work.